The Pectoralis Major is a muscle well loved by those who are into fitness, but is also a complex and convoluted muscle, much abused and often hypertonic.
The anatomy of the muscle is actually more complex than it first appears because the Pectoralis Major is a structure consisting of sheets, similar to a fan- positioned deck of cards, wrapped around the origin at the armpit.
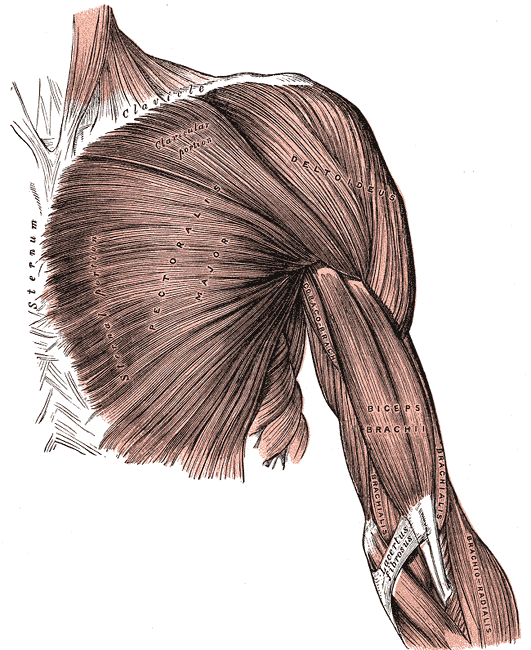
Roughly the Pectoralis Major can be divided into three sections: the clavicular section, the sternal section, and the costal section.
Symptoms of Pectoralis trigger points include chest pain, pait at the front of the shoulder, at inner arm (ulnar side), elbow and hand (ring finger and little finger). In addition, a trigger point in the lower edge of the right Pectoralis can even cause cardiac arrhythmia as demonstrated by Janet Travell (somatovisceral effect).
The myofascial syndrome of the Pectoralis Major is linked to heart problems in two ways: first, the symptoms of severe cases of trigger points of the Pectoralis Major are very similar to the painful symptoms of angina and cardiac ischemia (resulting in the possibility of wrong diagnosis at least as self-diagnosis of the terrified patient who thinks he has a heart attack), on the other, myocardial infarction tends to leave trigger points in the Pectoralis Major and therefore residual pain in the chest caused precisely by these satellite trigger points .
In addition, the taut bandelets caused by trigger points pull the shoulders forward and down. One consequence of this imbalance will be an overload of the anatomical posterior antagonists such as eg the Romboids, which then in the long run develop secondary trigger points being overloaded in bringing the shoulders back into a more neutral place .
It isinteresting to note that here as in other cases, when secondary trigger points are generated in antagonist muscles, usually it will be enough to deacivate the main trigger points to automatically obtain relief in the secondary trigger points, so for example releasing trigger points of the Pectoralis can often also improve chronic pain in the interscapular area as a consequence of the relief of the Rhomboids.
Other secondary trigger pointsmoreover may arise in the Sternocleidomastoid and Scalenes because in the head and neck are also take an unbalanced forward position. I will then be good practice to dealwith the Pecs, the Scalenes, the Sternocleidomastoids, and upper back muscles as the Rhomboids, since they are functional groups of agonists and antagonists, which tend to influence each other.
Causes
The Pectoralis Major rotate the arm internally and move it medially. They are usually hypertonic muscles especially when compared with the posterior antagonists, so even in the absence of real trigger points, there will often be a disharmony between them and their antagonists in people who practice physical culture. The stereotype is well known of the bodybuilder with huge pecs who can not even comb his hair behind his head.
It can also be said (at least for normal people!) that the human being lives "forward" due to the fact that the eyes scan fontally, so the majority of our psychological and even physical activities have a dynamism and resonance for the most part frontally. It istherefore natural to expect an greater exertion of certain muscles that perform the primary activities forward, and in particular of the chest.
Other causes are cardiac activity that finds resonance in Pectoralis due to viscerosomatic effect , and respiratory activity. Finally, a terrible cause for overexertion of chest muscles is the use of heavy backpacks, eg by students of school age. Truly, school can be bad for you!
Treatment
To successfully treat the trigger points of the Pectoralis Major, one should first be familiar with the complexities of this muscle. In practice, it is necessary to differentiate the different angles of the directions of the fibers of the clavicular section, the sternal section, and the costal section. Please note that the name of these three sections is given from the bone that unites medially, while all three, however, originate at the humerus laterally.
- Clavicular section. The fibers are directed diagonally from the inner half of the Clavicle toward the top of the Humerus downward. The central trigger points cause referred pain in the anterior Deltoid.
- Sternl section. The fibers are almost horizontal from the Sternum to the Humerus. Trigger points in this extensive area cause referred pain in the chest, inner elbow and hand of the same arm and therefore simulate angina attacks.
- Costal section. The fibers are directed diagonallyfrom the area of the fifth to seventh ribs upward toward the top of the humerus. Trigger points in the lateral edge of this lower section cause pain and hypersensitivity to breast and nipple with understandable concerns, especially in women afflicted. A specific point of the rib section of the right pectoral can cause instead cardiac arrhythmia. To locate this point, imagine a vertical line parallel to the sternum, which passes through the inner third of the clavicle. The intersection of the imaginary line with the intercostal space covered by the rib section of the Pectoralis is the area that should be explored to find that point.
Finally to complete the treatment of the Pectoralis Major, a stretching routine is an essential part. A good method is to help the stretch using e.g. the frame of a door by grasping it or placing high against it the inside of the bent elbow, and rotating the trunk to the opposite side. Hold the tension for at least a minute.