The group Psoas Major, Psoas Minor, Iliacus is another great unknown universe of our muscles, and as all beings who feel wrongly ignored, it often exacts bitter payment for this affront.
The group is called Iliopsoas because it begins at the top as two or three muscles (if the Psoas Minor is present, in about half of individuals), which inferiorly merge into a single muscle and tendon.
Before going into the study of exquisite suffering caused by our friend Iliopsoas, it will be good to do a simple consideration that, although elementary, will allow us to understand the problems that too often official medicine overly complicates, as well as hope to find the real, rational, radical ,simple remedy for related syndromes.
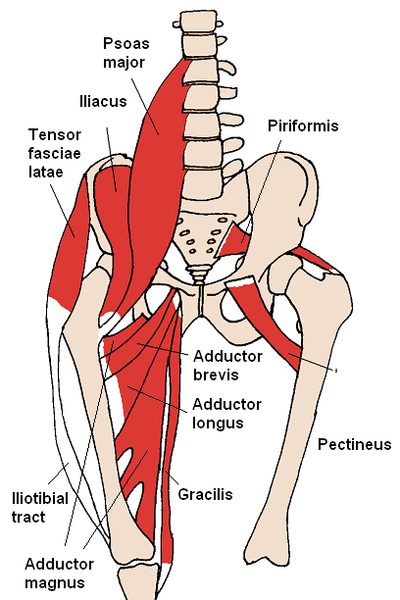
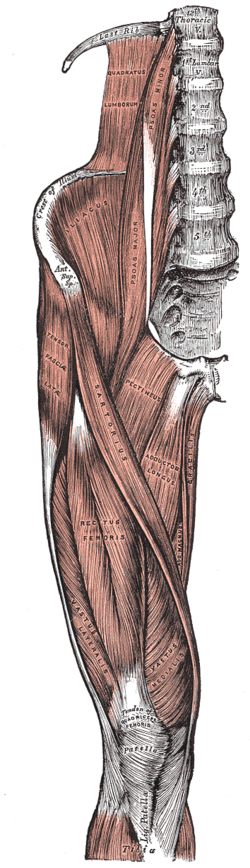
The consideration is as follows: let's observe the anatomical tables here reproduced and consider attention to the anatomy of the muscles involved. Then one will easily agree on the following findings:
1. the lumbar section of the spine has no ribs;
2. the Psoas is one of two major muscles that link the upper half of the body to the lower half (the other being the Quadratus Lumborum).
Now, from the fact that the lumbar spine does not have the rib cage, derives the result that the lumbar spine is subjected to much greater stress than the thoracic spine, which instead is aided and protected by the rib cage. Because the Psoas is one of the main muscles involved in such stress is logical to expect to find here significant developments regarding trigger points and pain and dysfunctional syndromes. And so it is. It should be noted in passing that the other muscle with lumbar support functions is the Quadratus Lumborum , which in fact is the other major responsible for lumbago and similar issues.
So because of the fundamental function of the Psoas Major, trigger points can be expected in it. Now let's imagine what happens when the Psoas contracts: because of his joining the trunk to the pelvis, a shortened Psoas compress the lumbar vertebrae and the lumbar intervertebral discs, and in extreme cases it will be real cause for disc herniations. Again, since there are no ribs at the lumbar level, there will not be other absorbing structures to counter such compression action from a contracted Psoas.
To get a graphic idea, imagine a series of coins placed one above the other and aligned vertically just as are the vertebrae and intervertebral discs. Imagine then to press the column of coins eccentrically, ie along an edge of the upper coins. What will happen is that the coins that protrude from the opposite side, will pop out from the column due to the applied pressure. Well, what is exactly what happens when a contract and Psoas infested with trigger points starts raising hell!
Here is revealed the cause of many "mysterious" herniated disc, those, to be clear, that arise without traumatic events or specific incidents, such as lifting a heavy weight awkwardly. Note that the Quadratus Lumborum can cause similar discopathies but since the latter muscle is located more laterally, then if the hernia protrudes sagittally (front or rear), the Psoas will be more responsible, but if the Quadratus is more involved, then you will find a more lateral compression.
Once the above is understood, then you will see how it is easily possible to reduce these disk hernias by simply releasing the trigger points and stretching the psoas with appropriate types of stretching (which will be discussed later), bearing in mind that unless one continues the program of stretching and manual therapy on an ongoing basis, the problem will almost inevitably reoccur because of daily stress and perpetuating factors.
Referred pain
In short: pain, very intense, along the lumbar spine down to the sacrum and buttock, with possible anterior pain at the groin and thigh.
In general, the pain caused by Psoas extends vertically along the lumbar spine and the sacrum can reach up to the chest area. If the Iliacus is involved, you may also have pain in the groin and thigh. In any case, the vertical distribution of pain helps to differentiate from referred pain from the Quadratus lumborum, which instead causes pain that extends horizontally in the lumbar area.
In acute cases, the pain attack can be incapacitating. In emergency cases, which tend to occur in the morning upon rising, one should walk on all fours and start immediately the stretching exercises that follow, then alternating with the self massage explained below.
Associated problems
A shortened and contract Psoas also increases in diameter. This can cause compression of the femoral , lateral femoral cutaneous, and genitofemoral nerves where they exit from the pelvis along with the muscle itself under the inguinal ligament. Sometimes also the Ilioipogastric and Ilioinguinal nerves penetrate the Psoas Major, and therefore a Psoas plagued by trigger points can give rise to several additional problems due to possible compression and irritation of these innervatures, in particular, the problems may involve the genitourinary system and the digestive system.
Anatomy and Physiology
The Psoas Major is attached superiorly along the sides of the thoracic vertebrae (T12) and lumbar (L1-L5) and related intervertebral disc. Inferiorly the tendon attaches to the Lesser Trochanter of the Femur.
The Psoas Minor if present instead attaches inferiorly to the pubic bone.
The Iliacus attaches superiorly to the upper two thirds of the iliac fossa. Inferiorly it joins the tendon of the Psoas, and in part directly attaches to the femur near the Lesser Trochanter.
It should be borne in mind that the joints crossed (and therefore the possible pain and dysfunctional problems) are: lumbar intervertebral, lumbosacral, sacroiliac, hip.
The primary function of the Iliopsoas is hip flexion. In addition, the Psoas contributes to the extension of the lumbar spine, thus increases the lordosis and a trained eye will recognize immediately a contracted Psoas looking from the side to a person who has the typical "duck" walk with pronounced lordosis, pelvis rotated forward, and hip flexion even at rest. To a lesser extent the Psoas and Iliacus contribute to abduction and lateral rotation of the thigh.
Activation of the trigger points
The trigger points in the Psoas can generally be activated in two ways, a traumatic event such as lifting a weight or bending, or a more subtle one, eg to sit habitually with the knees bent close to the chest or to alsayws sleep in a fetal position. As an example, in weightlifting, a classic situation of Psoas trigger point activation occurs when standing and using a heavy barbell for biceps: in this case the Psoas is contracted strongly and bilaterally to stabilize the spine. Then if you add a back and forth swinging motion of the body due to excessive weight, you undergo a high risk of disc herniation because to the contraction of the Psoas the oscillation of the column is added. So: use the alternate dumbbells to work the biceps and do not risk hurting yourself overloading the Psoas - using alternate dumbbells the load reduced by 50%,
Differential diagnosis
A Psoas plagued by trigger points can simulate visceral abdominal problems. The more widespread misinterpretation of such pain occurs when the right Psoas is involved. In this case a number of unnecessary appendectomies is performed in ignorance of the nature and extent of the myofascial pain. In addition, the Psoas may affect both the genitourinary system and the digestive system because of the nerves that a contracted and shortened Psoas may entrap. When the referred pain emerges mainly in the lower insertion of the muscle, one can also mistakenly think of hip joint problems. But probably the biggest erroneous diagnosis remains, at any rate, the one that sees in various disc problems the cause, rather than the effect caused by myofascial syndromes, of many of the painful lower back problems.
Therapy
To achieve the cure for the Psoas Myofascial syndrome, it is essential to attack the problem from three angles:
1. Manual technique
2. Stretching
3. Elimination of perpetuating factors
The Psoas may be a stubborn muscle, and the thought of solving the problem without addressing it in a comprehensive manner means illusion. On the other hand, in my personal opinion and personal experience, a number of risky surgeries for disc problems and back pain can be avoided by proceeding in the manner described below, in conjunction with a similar approach applied to the Quadratus Lumborum.
It is important to carry out a methodical examination of the patient to determine the effective involvement of the muscles and the gravity of the situation. First, it is necessary to consider restrictions on the movement of the extension of the thigh at hip level. Let the patient lie supine on the table with his legs dangling over the edge of the table. The patient then grasps the knee of the leg is not compromised and brings it to the chest for stabilization and to eliminate the lumbar lordosis. So you will have afflicted leg hanging free over the bottom edge of the bed. (Note: this position is also a way to make a nice lengthening or stretching of the Psoas, that you can use as preliminary stretching before the more intense one described below). At this point you will see one of the following possibilities:
1. the thigh does not fall below the horizontal plane, but the ankle hangs freely
2. the thigh falls below the horizontal plane and the ankle hangs freely
3. the thigh does not fall below the horizontal plane and the leg does not bend at the knee, but is extended
4. the thigh falls below the horizontal plane, but the leg does not bend at the knee and is extended
Now in case 1. and 3. the Psoas is tightly contracted, and in addition in case 3.,the knee extensors are also contracted, in particular the Rectus Femoris. In case 4. only the knee extensors are contracted, while in case 2. the situation is optimal and no decrease in range of motion is found either at the hip or knee.
Once the degree of restriction and the areas of restriction are establised by this observation, one will proceed to the identification and treatment by manual technique.
At the outset, the following anatomical structures should be identified:
1. Anterior Superior Iliac Spine (ASIS): easily palpable bony prominence on either side of the pelvis, roughly at a height midway between navel and pubic bone, to which the Inguinal Ligament attaches.
2. Rectus Abdominis: this is the abdominal muscles
3. Femoral Triangle: an area bounded superiorly by the Inguinal Ligament (connects the ASIS to the Pubic Bone), medially by the muscle Adductor Longus (see table) and laterally by the Sartorius muscle (see table)
Manual Technique
Essentially there are three areas to examine and treat, all reachable although partially, from the abdomen:
1. Psoas lumbar section located under the abdominal muscles and content (below the navel and lower abdomen)
2. area of the inner edge of Ilium behind the prominence of the Anterior Superior Iliac Spine (the bony protrusion of theepelvis at more or less the level of the appendix).
3. the area of the Lesser Trochanter (where the Femur joins the pelvis).)
To treat the lumbar section of the Psoas, it will be appropriate to place a support under the affected side of the supine patient, eg have the patient lying on the table partly rotated toward the opposite side, and slide some rolled towels or other suitable support under the side to be treated. With this precaution, the abdominal contents will move by the force of gravity to the opposite side of the lumbar spine and allow the hand, or extended fingers to sink into the abdomen diagonally from the outside toward the lumbar spine.
It is important to go slowly. Once you reach the Psoas, proceed with slow movements of the fingers back and forth horizontally (perpendicular to the column) and vertically (parallel to the column) for the whole extension of the abdomen (it is important to study te anatomical table to learn the extension of the muscle and try to cover as much territory as possible). It must be said that the Psoas is not fully reachable over its full extension, especially in overweight patients, but one must try to explore as much as possible. One should try to identify the points that reproduce the lumbar and groin pain, and their massage will be very beneficial even if the entire muscle can not be massaged.
To treat the iliac region, it will be good to abduct (open) the leg slightly and proceed with the fingers along the edge of the pelvis, pressing against the concavity of the Ilium (Iliac Fossa) and against the Iliac Crest, until the points that reproduce the pain are found. It will not be generally possible to explore much of the muscle.
To treat the area of the lower attachment of the Ileopsoas, will be useful also to slightly rotate the leg outward and explore the inner arch of the head of the Femur. In this case, the referred pain tends also to emerge in the groin and upper thigh region.
Stretching
In my experience, stretching can be the decisive factor in the Psoas issues, partly because of the obvious difficulties encountered in massaging it because there is no doubt that the muscle is not easy to access especially in certain physical types and in overweight people.
At the same time, many of the stretching exercises for the Psoas recommended by the authorities are not always adequately effective. For example, previously the stretching has been described consisting of letting the leg hang from the tablex. Well while in that caseone has a gentle stretching exercises, this lengthening is not entirely adequate to resolve an acute painful crises.
The more effective stretching more is similar to the Warrior position of yoga. It consists in a frontal position with the leg opposite to the side to stretch, being positioned forward and bent at the knee. The leg to be stretched is instead kept extended backwards. The position is called lunge in gymnastics. The Warrior yoga position (and the Archer positon as well) is modified in two basic details:
1. you should rotate your pelvis and torso forward in the direction opposite to the side to be stretched (and slightly tilt your torso back ("tails between their legs") to maximize groin stretch
2. you should rotate the posterior leg and foot (those of the side to be stretched) internally (inversion) around the same axis of the leg so that both feet point in the same direction, not in two perpendicular directions, as it happens in the classical Warrior position.
In this way you will have maximum elongation of the Psoas. It is essential to proceed very gradually to avoid overstretching the groin. Hold a mild stretch for at least a minute and only gradually increase the tension. It is possible to lean with the shoulder laterally against the wall while doing the exrcise, if one has trouble maintaining balance.
During an acute attack of Psoas pain repeat this stretching several times during the course of the day for 1-5 minutes each time. Be sure to apply the same stretch, perhaps for shorter periods, also to the opposite side for reasons of symmetry and balance.
Note: the other fundamental stretching for back problems is the yoga position of the Triangle or Trikonanasa. This position stretches the Quadratus Lumborum and if practiced along with the Psoas stretching just described, will be of great help for problems with low back pain, lumbago, sciatica, herniated discs, and the like.
Perpetuating Factors
Unless one methodically identifies and eliminates the factors that initiate or contribute to the syndrome, the problem will almost certainly reoccur in the medium term.
An important factor in Psoas problems is that the Psoas works to stabilize the pelvis, so it opposes forces that tend to rotate the hips around the axis passing through the hips themselves. The largest of these forces is frequently represented by contracted Hamstrings. Then we can deduce how often, the true source of the Psoas problem is to be found in the trigger points of the leg extensors (muscles in the back of the thigh). It is therefore essential to achieve true cure, to treat the trigger points along theBiceps Femoris as well as those of the Gluteus because otherwise the Psoas will soon fall under the same conditions of stress caused by his antagonists.
Other perpetuating factors may be the habit of sitting down with one's knees close to the chest, as well as the habit of always sleeping in a fetal position with knees bent at an acute angle near the trunk.
Finally, as explained above, certain ways to lift weights, which call into action a strong contraction of the Psoas because of using the leverage of the forearms instead of employing the load-bearing function of column, like for example standing biceps curls using a heavy barbell, expose to great risk of causing Psoas trigger points as well as a true herniated lumbar discs. In such cases one should try to reduce the weight or if heavy weight is desired, one can use dumbbells while alternating the flexion of the biceps in order to reduce the load by 50%.